Abstract
Exposure surrogates, such as air quality measured at a fixed-site monitor (FSM) or residence, are typically used for health estimates. However, people spend various amounts of time in different microenvironments, including the home, office, outdoors and in transit, where they are exposed to different magnitudes of particle and gaseous air pollutants. Health risks caused by air pollution exposure differ among individuals due to differences in activity, microenvironmental concentration, as well as the toxicity of pollutants. We evaluated individual and combined added health risks (AR) of exposure to PM2.5, NO2, and O3 for 21 participants in their daily life based on real-world personal exposure measurements. Exposure errors from using surrogates were quantified. Inter- and intra-individual variability in health risks and key contributors in variations were investigated using linear mixed-effects models and correlation analysis, respectively. Substantial errors were found between personal exposure concentrations and ambient concentrations when using air quality measurements at either FSM or the residence location. The mean exposure errors based on the measurements taken at either the FSM or residence as exposure surrogates was higher for NO2 than PM2.5, because of the larger spatial variability in NO2 concentrations in urban areas. The daily time-integrated AR for the combined PM2.5, NO2, and O3 (TIARcombine) ranged by a factor of 2.5 among participants and by a factor up to 2.5 for a given person across measured days. Inter- and intra-individual variability in TIARcombine is almost equally important. Several factors were identified to be significantly correlated with daily TIARcombine, with the top five factors, including PM2.5, NO2 and O3 concentrations at ‘home indoor’, O3 concentrations at ‘office indoor’ and ambient PM2.5 concentrations. The results on the contributors of variability in the daily TIARcombine could help in targeting interventions to reduce daily health damage related to air pollutants.
1. Introduction
Adverse health effects of air pollution are a major public health issue globally. The World Health Organization (WHO) estimated that over 80% of the population living in urban areas breathes where the air quality does not meet the WHO guidelines [1]. Exposure to air pollution is related to numerous types of health damage. Exposure to daily PM2.5 concentrations has a causal relationship with cardiovascular illnesses and premature mortality [2]. There is a causal relationship between short-term exposure to 1 h NO2 concentrations and respiratory disease outcomes [3]. Exposure to an 8 h daily maximum ambient O3 concentration is causally associated with respiratory illness [4].
A number of epidemiological studies have estimated the health risk of air pollution based on fixed-site monitor (FSM) as a surrogate for exposure because of readily available real-time data with high measurement accuracy [5,6,7,8,9]. People typically spend over 85 percent of their time in indoor environments where they are usually exposed to different levels of concentrations than ambient concentrations [10]. For example, Che et al. [11] demonstrated that, at school, the mean exposure error from using outdoor PM2.5 concentrations at FSM as a surrogate was up to 30%. Some studies estimated exposure based on static residence-based approach (e.g., land use regression approach) to model people’s exposure to air pollution using nearby monitoring stations at residential addresses [12,13,14,15]. However, exposure concentration varies among microenvironments (e.g., ‘home indoor’, ‘office indoor’, ‘others indoor’, ‘outdoor’ and ‘transit’) [16,17]. For example, Koehler et al. [17] demonstrated that PM2.5 exposure concentrations substantially varied across different microenvironments with a geometric mean of 8.0 µg/m3 at home, 2.4 µg/m3 at work, 6.8 µg/m3 in transit, 8.4 µg/m3 at an eatery and 4.9 µg/m3 in other microenvironments. The residence-based approach is unable to capture the variation in air pollution exposure across different microenvironments because it ignores human mobility and does not properly apprehend the space-time dynamics of air pollution [18]. Thus, the residence-based approach as a surrogate may lead to a bias in the exposure-response relationship. Little is known about the exposure error between a surrogate and real-world exposure concentrations.
The health risk of exposure to air pollution depends on the exposure concentration over time in a microenvironment that leads us to quantify time-integrated or personal exposure across the microenvironments [19]. Personal exposure to air pollution is defined as the product of the average personal exposure concentration in a microenvironment and the total time spent in that microenvironment [16]. To date, some studies quantified the variability of personal exposure to air pollution across different microenvironments for a single pollutant [16,20,21,22]. For example, Mazaheri et al. [16] investigated the variability of personal PM2.5 exposure across different microenvironments and activities among 14 adult participants in Queensland, Australia. However, people are typically exposed to a mixture of particle and gaseous pollutants simultaneously in the real world. Each air pollutant is different in terms of health risk and toxicity, which leads us to quantify personal exposure to combined particle and gaseous pollutants. To our best knowledge, no study has been conducted to quantify overall exposure variability for combined personal PM2.5, NO2 and O3 exposure concentrations across the microenvironments to date.
Because an individual’s mobility varies in location and time, exposure concentrations may differ widely between individuals and over time for a given individual [23,24,25]. Previous studies have demonstrated the inter- and intra-individual variability in personal exposure concentrations for single pollutants [25,26,27,28]. In Guangzhou, China, variance component analysis demonstrated that the intra-individual variability was 90% in the daily lognormal personal PM2.5 exposure concentrations measured in 16 adult subjects [26]. In contrast, Chen et al. [27] reported that inter- and intra-individual variability in personal PM2.5 exposure concentration were almost equal. For NO2, Lee et al. [29] demonstrated that the intra-individual variability was higher than inter-individual variability in daily exposure concentrations. Grivas et al. [30] reported that the inter- and intra-individual variability were almost similar (51–56% intra-individual variability across the cities) in weekly average O3 exposure concentrations among school children in two cities, Athens and Thessaloniki, in Greece. However, because people are exposed to multiple pollutants simultaneously, it is important to quantify inter- and intra-individual variability and the key contributors of variability in the combined exposure to PM2.5, NO2 and O3 concentrations. No information is available on the inter- and intra-individual variability in the combined exposure to PM2.5, NO2 and O3, and the key contributors affecting the variability. Identifying and characterizing the key contributors of inter- and intra-individual variability in combined PM2.5, NO2 and O3 exposure may help in targeting interventions to reduce the health effects of exposure to a mixture of air pollutants.
The concentrations of different pollutants cannot be added directly to quantify combined exposure due to their differences in sampling units and their toxicity in terms of health risks. To overcome this limitation, an added health risk (AR) model had been applied in this study which was developed by Wong et al. [31] as the basis of the multipollutant air quality health index (AQHI), considering local hospital admissions data for the 3 h moving average of individual air pollutants. The AQHI approach is used by the Hong Kong Environmental Protection Department (HKEPD) to provide advice to the public regarding short-term health risks of air pollution [32] and was also used in our previous study to evaluate the impacts of ambient concentration changes due to emission control measures in Hong Kong [33]. In this study, we would use the same method to combine the health risks from multiple pollutants and assess the inter- and intra- individual variability in terms of the time-integrated health risk.
The objectives are to: (1) quantify the exposure error for PM2.5, NO2 and O3 between personal exposure concentrations across the selected microenvironments and ambient concentration from the FSM and residence location; (2) quantify the time-integrated AR (TIAR) for the combined PM2.5, NO2 and O3 exposure concentrations for each participant on each measured day and its contributions from selected microenvironments; and (3) identify key contributors of inter- and intra-individual variability in TIAR.
2. Materials and Methods
This section describes: the study design for personal exposure concentration measurements; the instrumentation for air quality measurements; the time-location record of the participants; the exposure error estimation between personal exposure concentrations and ambient concentrations; the calculation of health risk; time-integrated health risk; and inter- and intra-individual variability in TIAR for PM2.5, NO2, and O3 and combined PM2.5, NO2, and O3 exposure concentrations.
The supplementary material contains additional details on: (a) sensors specifications that are used to measure personal exposure concentrations; (b) carbon dioxide as an indicator of microenvironments to check the consistency of the recorded time-location patterns of the individual; (c) sensitivity analysis of AR estimation based on 1 min exposure concentrations of the pollutants instead of 3 h moving average concentrations; and (d) quantification of inter- and intra-individual variability in the daily time spent in each microenvironment.
2.1. Study Design
To quantify the health risk of combined personal exposure to particle and gaseous pollutants across the selected microenvironments, a longitudinal study was conducted among twenty-one participants. All participants were recruited from faculty, staff, and postgraduate students from the Hong Kong University of Science and Technology, Hong Kong. The participants lived in different districts and areas across Hong Kong, including urban and suburban areas. The air quality of Hong Kong is influenced by local emission sources, including on-road motor vehicles, power plants and marine vessels [33], and regional air pollution from mainland China [34]. Each participant performed the continuous air quality measurement on multiple consecutive days based on their availability, with an average of five days. Data were collected for 106 person-days. During the personal monitoring campaigns, the outdoor air quality of residences was also measured for seven participants. Demographic information (e.g., age, occupation, number of occupants at home, living floor, smoking) and residential characteristics (e.g., type of ventilation status at home, AC type, type of cooking stoves, cooking duration per day and frequency of floor cleaning) were collected using a web-based structured questionnaire.
2.2. Instrumentation
The PM2.5, NO2, and O3 exposure concentration were measured across the microenvironments that were visited by the participants. As an indicator of indoor and outdoor differences, CO2 concentrations were also measured. PM2.5 concentrations were measured using a photometer Aerocet 831 Handheld Particle Counter (Metone, Grants Pass, OR, USA) for personal exposure concentration across the microenvironments and a photometer model 212 Ambient Particulate Profiler (Metone, Grants Pass, OR, USA) for outdoor air quality at residence locations. The concentrations of O3 and NO2 were measured using electrochemical sensors that were the model B series from Alphasense, Braintree, UK. The CO2 concentration was measured using a nondispersive infrared Premier CO2 sensor from Dynament, Mansfield, UK. The sensors of all pollutants were integrated into a portable system called Portable Air Station (PAS) and an outdoor portable system called a Mini Air Station (MAS) [35,36]. The PAS was used to measure personal exposure concentrations across the microenvironments (Figure 1). The PAS was able to store local data and transmit data to a server in real-time.
Figure 1.
Real-time (24 h) personal air quality measurement using portable air sampler.
The sensors measured air pollution concentrations at 1 min resolution. The PAS has 12 V Li-ion Battery inside for a standby capacity of more than 10 h. The PAS has rolling wheels that make the 15 kg PAS convenient to move from one place to another with participants. Participants were instructed to always carry the instrument and keep the instrument within 1 m of them in indoor environments (e.g., home and office). Participants were given some flexibility to keep the PAS in a nearby safe place while taking a bath.
Details of the quality assurance (QA) and quality control (QC) for the sensor measurements are provided elsewhere [36,37,38]. The accuracy of the sensors used in PAS and MAS were evaluated based on measurements with standard gas at known concentrations in the laboratory and collocation with reference methods at the government operated Air Quality Monitoring Station (AQMS) at Mong Kok. The differences in concentration measurements between the reference methods and sensors were, on average, less than 1% for PM2.5 and NO2, and about 4% for O3 over 350 sampling hours [38]. During air quality measurements and post data analysis, QA and QC were maintained to obtain a high quality of data. Detailed procedures regarding the QA and QC for air quality data are published elsewhere [39].
2.3. Time-Location Records
Participants recorded the start and end times of each location that they visited and categorized each location into one of the five predefined microenvironment categories using the aTimeLogger app on their smartphone (Available online: http://atimelogger.com, accessed on 20 December 2021). The five categories of microenvironments were: ‘home indoor’, ‘office indoor’, ‘others indoor’, ‘outdoor’, and ‘transit’. Two participants recorded their time-location information in open text on their smartphones. Participants were asked to record their time-location immediately after changing each microenvironment to avoid misclassification of time-location information.
CO2 is produced by human exhalation as a function of metabolic processes [40]. The outdoor CO2 concentration level is lower than the CO2 concentration in indoor environments because of human occupancy [41]. Based on our analysis, CO2 concentration substantially varied between indoor and outdoor microenvironments and among different indoor microenvironments depending on the occupancy number and ventilation condition, provided in supplementary material. Therefore, we used real-time CO2 concentration time-series (1 min resolution) in this study to check the consistency of the recorded time-location patterns of the individual.
2.4. Quantification of Exposure Error between Personal Exposure Concentrations and Ambient Concentrations
To compare personal exposure concentrations with the ambient concentration at the residence location, the outdoor air quality was measured at seven participants’ residences. The MAS was used to measure residences’ outdoor air quality. The MAS was placed on the balcony or another outdoor space of the residence.
Hourly-average ambient concentrations of PM2.5, NO2 and O3 were retrieved from FSM stations of the Hong Kong Environmental Protection Department (HKEPD). FSM stations were selected based on the nearest distance to the participant’s resident address.
The exposure error between personal exposure concentrations and ambient concentrations was estimated as below:
where EEp,j,i is the exposure error (%) in daily average concentration between personal exposure concentration and ambient concentration of pollutant p in each person-day j for participant i. PCp,j,i is the daily average personal exposure concentrations of pollutant p in each person-day j for participant i. ACp,j,i,l is the daily average ambient concentrations of pollutant p in each person-day j for participant i at location l (i.e., nearest FSM or residence location).
2.5. Calculation of Health Risk
For a mixture of PM2.5, NO2 and O3, AR of hospital admission for respiratory diseases (International Classification of Disease codes 460-519) and cardiovascular diseases (International Classification of Disease codes 390-459) for all ages were quantified [31]. Although AR in AQHI was quantified hourly based on a 3 h moving average of ambient concentrations [31,32], we estimated AR based on continuous 1 min personal exposure concentrations. This is because we quantified AR in each microenvironment across the person-days, and participants spent less than 3 h in some of the microenvironments. Thus, 3 h moving average concentrations may cause misrepresentation of those microenvironments by averaging before and after the microenvironmental concentrations. Based on our analysis, the median differences of the daily average AR estimation between 1 min exposure concentrations and 3 h moving average concentrations were less than 2% for each pollutant, regardless of the microenvironments. For each pollutant (ARp) in the mixture, AR is quantified:
where Cpt is the 1 min personal exposure concentration (µg/m3) of pollutant p at time t, and βp is a regression coefficient in units of (µg/m3)−1 of pollutant p. Wong et al. [31] reported the values of βp based on time series analysis, including βPM2.5 = 2.1 × 10−4 per µg/m3, βNO2 = 4.5 × 10−4 per µg/m3 and βO3 = 5.1 × 10−4 per µg/m3.
ARp = [exp(βp.Cpt) − 1] 100%
The AR for a mixture of PM2.5, NO2, and O3 is quantified:
where ARcombine is the sum of the AR for PM2.5, NO2 and O3 concentrations
ARcombine = ARPM2.5 + ARNO2 + ARO3
2.6. Time-Integrated Health Risk
Because the health risk of air pollution depends on the exposure concentration over time in a microenvironment, the contribution of each microenvironment to the daily health risk was estimated based on TIAR. The TIAR for a mixture of PM2.5, NO2 and O3 across the microenvironments for a participant was estimated as
where, is time-integrated ARcombine (%h) in microenvironment k in person-day j exposed by participant i for the AR of combined PM2.5, NO2 and O3; is the average ARcombine (%) in microenvironment k for participant i in person-day j; is the duration (hour) spent in microenvironment k by participant i in person-day j; and n is the total number of microenvironments. This approach of estimating the TIAR in a given microenvironment is similar to the method for estimating time-integrated exposure in a microenvironment used by Klepeis [42].
We also quantified TIAR across the microenvironments for the individual pollutant, i.e., PM2.5, NO2 and O3 exposure concentrations:
where, is time-integrated ARp (%h) in microenvironment k in person-day j exposed by participant i for the pollutant p; is the average ARp (%) in microenvironment k for participant i in person-day j for pollutant p.
To quantify which microenvironments contribute disproportionately, the health risk relative intensity was estimated. Health risk intensity was calculated by dividing the fraction of the health risk for a participant exposed in a microenvironment by the time fraction of the day that the participant spent in that microenvironment. The approach of calculating health risk intensity is similar to the approach for calculating the dose relative intensity estimation used by Mazaheri et al. [43].
where, is the health risk intensity in microenvironment k in person-day j for participant i; is the total time-integrated ARcombine (%h) on a given day of j for participant i; is total time spent (hour) in microenvironment k in person-day j for participant i; and is total spent on a given day of j for participant i. A relative intensity value greater than one for a microenvironment suggests that the fraction of the TIARcombine was higher than the time spent in that microenvironment. A value smaller than one indicates that the fraction of the TIARcombine was less than the fraction of the time spent in that microenvironment.
2.7. Quantifying Inter- and Intra-Individual Variability in Time-Integrated Health Risk
To quantify proportions of inter- and intra-individual variability in the daily total TIAR, variance component analysis was used. Variance component analysis in the daily total TIAR was performed separately for PM2.5, NO2 and O3, and combined PM2.5, NO2 and O3. To quantify the variance component, a linear mixed-effects model with only a random intercept was developed [17,25]:
where Zij is the log-transformed daily total TIAR for PM2.5, NO2 and O3, and combined PM2.5, NO2 and O3 in person-day j for participant i; μ is the fixed mean (logged) TIAR for all subjects; and εij is the error. In linear mixed-effects models, a person-specific random effect bi assumed to be normally distributed with zero mean and variance (the inter-individual variability). The error εijp is assumed to have normal distribution with zero mean and variance (the intra- variability). The variance components for inter- and intra-individual were estimated using the method of restricted maximum likelihood (REML) [44].
Zij = µ + bi + εij
Intra-class correlation coefficients (ICC), i.e., the proportion of total variability attributable to inter-individual variability, was estimated as [45]:
To identify key contributors affecting the inter- and intra-individual variability in daily TIARcombine, we performed correlation analysis between TIARcombine and selected independent variables. The variables were the daily time spent at ‘home indoor’, ‘office indoor’, ‘others indoor’, ‘outdoor’, and ‘transit’; the daily average PM2.5 concentrations at ‘home indoor’, ‘office indoor’, ‘others indoor’, ‘outdoor’, and ‘transit’; the daily average NO2 concentrations at ‘home indoor’, ‘office indoor’, ‘others indoor’, ‘outdoor’, and ‘transit’; the daily average O3 concentrations at ‘home indoor’, ‘office indoor’, ‘others indoor’, ‘outdoor’, and ‘transit’; and the daily average ambient PM2.5, NO2 and O3 concentrations. The variables were averaged daily and for each participant in order to analyze correlation with the daily TIARcombine and participant-wise average TIARcombine, respectively.
2.8. Statistical Analysis
The normality of the distribution of data was checked using the Shapiro–Wilks test. For non-normal distribution, the Mann–Whitney test was used to determine the statistical significance of the difference between two independent groups. The Kruskal–Wallis test was used to compare more than two independent groups.
3. Results
The results include study participants and the time-location pattern; exposure error between personal exposure concentrations and ambient concentrations; time-integrated health risk across the selected microenvironments; and inter-individual and intra-individual variability in the time-integrated health risk.
The supplementary material contains additional results for (a) general characteristics of the study participants; (b) inter- and intra-individual variability in the daily time spent by participants in each microenvironment; (c) summary statistics of personal exposure concentrations of PM2.5, NO2 and O3 in each microenvironment across the participants; and (d) the relationship of ambient PM2.5, NO2 and O3 concentrations between FSM and the residence location.
3.1. Study Participants and Time-Location Pattern
General characteristics of the participants are given in the supplementary material. Twenty-one participants aged 21–60 years old participated in the longitudinal measurement of the health risk of personal exposure study. All of the participants are non-smokers and lived in non-smoking homes.
The mean daily percent of time spent by participants across the microenvironments are provided in Table 1. Participants spent, on average, only 2.5% of their daily time in an ‘outdoor’ environment. Among the five categories of microenvironments, participants spent most of their daily average time in the ‘home indoor’ (range: 9.3–24.0 h), followed by the ‘office indoor’ (range: 0–13.9 h), the ‘others indoor’ (range: 0–7.5 h), in transit (range: 0–5.8 h) and in the ‘outdoor’ (range: 0–4.6 h) microenvironment. Based on variance component analysis (given in supplementary material), intra-individual variability in daily time spent in all selected microenvironments ranged from 59% to 91%. Inter-individual variability was from 9% to 41% across the microenvironments. This indicates that the day to day variability in the time spent for a given individual in a microenvironment is higher than the differences in the average time spent in that microenvironment between individuals during the whole measurement period.

Table 1.
Daily time spent (hour) across the selected microenvironments (N = 106).
3.2. Exposure Error between Personal Exposure Concentrations and Ambient Concentration
The error percentage between the daily average personal exposure concentrations and ambient concentration for PM2.5, NO2 and O3 are provided Figure 2, where Figure 2A indicates the ambient concentrations from FSM and Figure 2B indicates the ambient concentrations from the residence location.
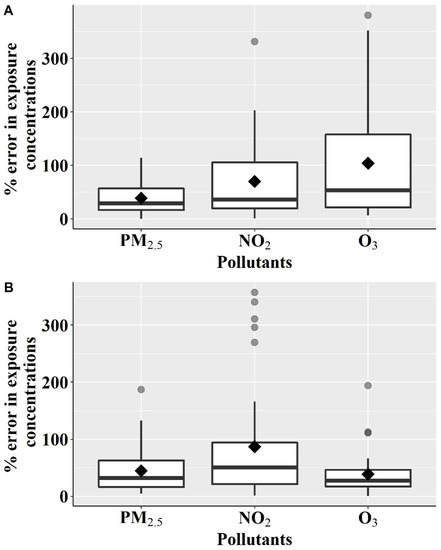
Figure 2.
Percentage error in daily average exposure concentrations of PM2.5, NO2 and O3 between personal exposure concentrations across the different microenvironments and ambient concentrations: (A) ambient concentrations from fixed-site monitors nearby the participant’s residence (N = 106); (B) ambient concentrations at residence location (N = 35).
When ambient concentrations were based on FSM, the mean error percentage was 39% and 70% for PM2.5 and NO2 concentrations, respectively. In comparison, the mean errors were 45% for PM2.5 and 87% for NO2 when ambient concentration was based on the residence location. This exposure error is primarily because of the spatial variability of the concentrations due to the daily movement of the participants across the microenvironments. The mean exposure error of NO2 was higher than PM2.5 when based on either the measurements at FSM and residence as exposure surrogates because of larger the spatial variability in NO2 concentrations in urban areas. The coefficient of determination (R2) values between daily average concentrations at FSM and the residence location was lower for NO2 (0.25) than PM2.5 (0.87) (this is provided in the supplementary material), indicating the larger spatial variability of NO2 concentrations.
For O3, the mean exposure error was 104% based on the air quality measurements at FSM and 39% based on the measurements at the residence location. This is because people are exposed to lower levels of personal exposure concentrations in different microenvironments than outdoors. For example, on a given person-day, the average personal O3 exposure concentrations were 27 µg/m3 in ‘home indoor’, 37 µg/m3 in ‘office indoor’, 25 µg/m3 in ‘others indoor’, and 17 µg/m3 in ‘transit’, while the daily average ambient O3 concentration on that day was 61 µg/m3 at FSM. The mean O3 exposure error using FSM was higher than using the residence location. This is because FSM used in our study is general FSM located at the top of the roof and not adjacent to busy roads. Thus, we measured higher O3 concentrations at FSM. In contrast, the participants live in urban areas close to busy roads, where an abundance of nitric oxide (NO) from on-road vehicles titrate O3 concentrations [33]. Thus, lower O3 concentrations were measured at residence locations.
The exposure errors based on FSM or residence locations were consistent for PM2.5 and lower than 50%, indicating small spatial variability in PM2.5 concentrations, similar to the previous study [46,47]. For NO2, exposure errors were higher (≥70%) because of larger spatial variability and were consistent throughout, based on FSM and residence locations. This indicates that NO2 exposure concentrations based on a single location either FSM or residence location cannot represent the large spatial variability in personal exposure concentrations across the microenvironments. For O3, exposure errors were inconsistent between FSM and residence locations because of O3 titration by NO. Thus, the results of exposure errors in NO2 and O3 concentrations as a surrogate highlights the importance of real world personal exposure concentration measurements with the daily active lifestyle of the individuals.
3.3. Contribution of the Selected Microenvironments in Time-Integrated Health Risk
The mean percent of the daily time-integrated health risk for combined PM2.5, NO2 and O3 exposure concentrations in each selected microenvironment are given in the supplementary material. There were significant differences (p < 0.001) in the median TIARcombine among the microenvironments. The daily highest TIARcombine (mean ± standard deviation, SD) 64% (±19%) was in the ‘home indoor’ microenvironment, where participants spent an average 66% (±17%) of their total daily time. The daily minimum TIARcombine 5% (±5%) was in the ‘outdoor’ microenvironment, where participants spent an average of 3% (±3%) of their daily time. Although ARcombine in ‘home indoor’ microenvironments was lower than the ‘others indoor’, ‘outdoor’ and ‘transit’ microenvironments, TIARcombine in ‘home indoor’ were found to be higher than those microenvironments due to the long dwelling time of the participants in the ‘home indoor’ microenvironment.
Because TIARcombine is related to the duration spent in each microenvironment, health risk intensities provide a clear picture of which microenvironment contributes disproportionately to daily health risk. Figure 3 presents the average health risk intensities in each microenvironment.
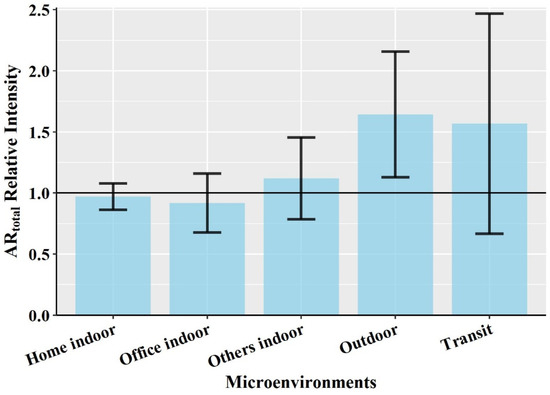
Figure 3.
Average time-weighted short-term health risk intensities in each microenvironment. Error bar represents standard deviation (Sample size, home indoor = 106, office indoor = 86, others indoor = 82, outdoor = 85 and transit = 78).
The maximum average health risk intensity 1.64 (±0.52) was found in ‘outdoor’ followed in order by ‘transit’, ‘others indoor’, ‘home indoor’ and ‘office indoor’ microenvironments. Among the microenvironments, intensity values exceeded 1 for the ‘outdoor’, ‘transit’ and ‘others indoor’, which indicated the fraction of TIARcombine in those microenvironments was higher than the faction of time spent in the corresponding microenvironments. This means that, although participants spent only a small fraction of their time in these settings, these microenvironments contribute disproportionately to ARcombine because of the elevated concentrations of pollutants. Thus, these microenvironments with large health risk intensity could help to prioritize interventions to reduce the daily health risk. Higher health risk intensity for combined PM2.5, NO2 and O3 exposure in the ‘transit’ microenvironment than in the ‘home indoor’ and ‘others indoor’ was because of the much higher NO2 concentrations in the vehicle’s cabin. Although PM2.5 and O3 concentrations in ‘transit’ were lower than ‘home indoor’ and ‘others indoor’ microenvironments, the higher health risk posed by NO2 offset the lower health risk of PM2.5 and O3 concentration. Among the two main microenvironments, ‘home indoor’ and ‘office indoor’ where participants spend most of their daily time, health risk intensity in the ‘office indoor’ microenvironment was much less than in the ‘home indoor’ microenvironment. This is because the average concentration for PM2.5 and NO2 in ‘office indoor’ microenvironments were always encountered as lower than the ‘home indoor’ microenvironment. The ‘office indoor’ was operated with a centralized mechanical ventilation and air-conditioned system with high-efficiency filters for particles (Minimum Efficiency Reporting values of 13, MERV 13), whereas the ‘home indoor’ microenvironment was commonly ventilated by opening windows which introduce more infiltration of outdoor pollution than the office. In addition, home is intensely influenced by indoor emission sources, including cooking and cleaning inside of the home. For example, Baxter et al. [48] found that cooking for more than an hour per day was significantly associated with a 5.7 µgm−3 increase in indoor PM2.5 concentrations compared to less than an hour per day.
3.4. Inter-Individual and Intra-Individual Variability in Time-Integrated Health Risk
Inter- and intra-individual variability of daily TIAR for PM2.5, NO2 and O3 and combined PM2.5, NO2 and O3 exposure concentrations across the microenvironment is given in Figure 4.
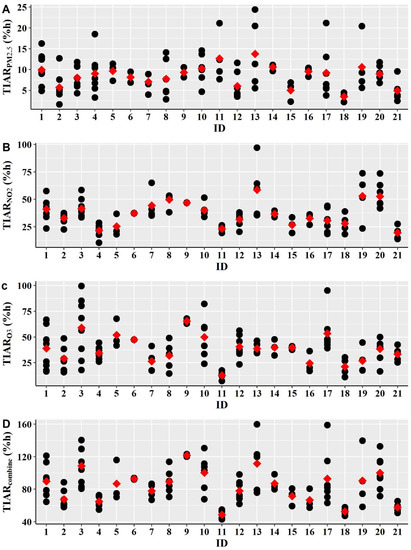
Figure 4.
Inter and intra-individual variability of the daily time-integrated health risk (TIAR) for (A) PM2.5; (B) NO2; (C) O3; and (D) combined PM2.5, NO2 and O3 exposure concentrations across the selected microenvironments. Black circle represents the total TIAR across the selected microenvironments in each person-day. Red square indicates mean of the TIAR for a participant.
The results demonstrated that there was substantial inter-individual variability in mean TIAR by a factor of 3.9 for TIARPM2.5, 3.0 for TIARNO2, 5.1 for TIARO3 and 2.5 for TIARcombine across the participants. Intra-individual variability indicates the daily fluctuations of TIAR that vary temporally from day to day. Large intra-individual variability in TIARPM2.5, TIARNO2, TIARO3 and TIARcombine was found in many participants. For example, the daily total TIARcombine varied by a factor up to 2.5 across the person-days of a given person. TIARPM2.5, TIARNO2 and TIARO3 varied by a factor of up to 7.8, 3.1 and 5.6 for a given person across the measured days, respectively.
Table 2 shows the variance component for inter- and intra-individual variability in lognormal daily TIAR for each pollutant and for combined PM2.5, NO2 and O3. The inter- and intra-individual variability between particle and gaseous pollutants was substantially different from each other. For TIARPM2.5, intra-individual variability (78%) was substantially higher than inter-individual variability (22%). This indicates that the daily personal activities and lifestyle of the participants are more important than where the participants live because of the small spatial variability in PM2.5 concentration. Thus, an individual has the potential to reduce PM2.5-induced health risk by modifying their daily activities and lifestyle. In contrast, for gaseous pollutants, inter- and intra-individual variance in both TIARNO2 and TIARO3 were comparable. Because of the larger spatial variability of gaseous pollutants than PM2.5, where participants live is important to reduce health risk for NO2 and O3 exposure. The larger inter-individual in TIARNO2 indicates that the health risk and sources of NO2 concentrations are widely varied across the participants. For TIARcombine, inter- and intra-individual variability is almost equally important. Thus, for combined PM2.5, NO2 and O3 exposure, both daily personal activities and a participant’s location are important to reduce health damages of air pollution exposure.
Table 2.
Proportion of inter- and intra-individual variability of time-integrated short-term health risk for each individual and combined pollutants.
Identified key contributors affecting inter- and intra-individual variability in TIARcombine are provided in Table 3. For inter-individual variability, TIARcombine was significantly (p < 0.05) correlated with PM2.5, NO2 and O3 exposure concentration at ‘home indoor’ microenvironments, PM2.5 and NO2 at ‘others indoor’ microenvironments, O3 at ‘office indoor’ microenvironments and ambient PM2.5 concentrations. Based on an interpretation of the correlation coefficient by Schober et al. [49], exposure to O3 concentration at ‘home indoor’ microenvironments was strongly correlated (r = 0.74, p < 0.001) with TIARcombine. There was a moderate correlation (i.e., 0.45 to 0.60, p < 0.05) of TIARcombine with PM2.5 and NO2 concentration at ‘home indoor’ microenvironments, PM2.5 and NO2 at ‘others indoor’ microenvironments, O3 at ‘office indoor’ microenvironments and ambient PM2.5 concentrations.
Table 3.
Correlation between time-integrated health risk of combined PM2.5, NO2 and O3 exposure concentrations (TIARcombine) and selected variables.
For intra-individual variability, TIARcombine was strongly correlated (r = 0.76, p < 0.001) with O3 concentration at ‘home indoor’ microenvironments and moderately correlated (i.e., 0.40 to 0.59, p < 0.05) with PM2.5 and NO2 concentration at ‘home indoor’ microenvironments, NO2 in ‘others indoor’ and ‘transit’ microenvironments, O3 at ‘office indoor’ microenvironments, and ambient PM2.5 and O3 concentration. There was also a weak but statistically significant correlation (i.e., 0.20 to 0.33, p < 0.05) of TIARcombine with time spent at ‘home indoor’ microenvironments, PM2.5 and O3 at ‘others indoor’ microenvironments, PM2.5, and NO2 and O3 at ‘outdoor’ microenvironments. These key contributors of intra-individual variability indicate that individual has great potential to reduce their health damage related to combined exposure to mixed particle and gaseous pollutants.
4. Discussion
To our best knowledge, this study is new in that is quantifies the health risk for combined personal PM2.5, NO2 and O3 exposure concentrations across different urban microenvironments, including ‘home indoor’, ‘office indoor’, ‘others indoor’, ‘outdoor’ and ‘transit’ microenvironments. Because health risk intensities are greater than 1 in ‘others indoor’, ‘outdoor’ and ‘transit’ microenvironments, these microenvironments contribute disproportionately to the daily health risk for combined personal PM2.5, NO2 and O3 exposure concentrations. This indicates that there are potentials to reduce individual’s daily health damage related to air pollution by minimizing exposure time in those microenvironments. The highest health risk intensity in ‘outdoor’ microenvironments indicates that sensitive people should avoid outdoor exposure for a longer time during high air pollution episode days. This is because the outdoor air quality in Hong Kong is contributed to by both local emission sources (e.g., on-road vehicles, marine vessels, and power plants) and regional air pollution [33,34]. People can use smart technology to check their health risk associated with outdoor air pollution, such as the Hong Kong AQHI App (Environmental Protection Department, Hong Kong) [32], Personalized Real-Time Air Quality Informatics System for Exposure—Hong Kong (PRAISE-HK) App (Hong Kong University of Science and Technology, Hong Kong) [50], AirVisual App (IQAir, Goldach, Switzerland) [51], Air Quality Index, Pollen and Fires—BreezoMeter App (BreezoMeter, Haifa, Israel) [52], Air Matters App (Air Matters Network Pty Ltd, Goldach, Switzerland) [53], ZephAir App (United States Department of State, Washington DC, USA) [54] and Plume Labs Air Quality App (Plume Labs, Paris, France) [55]. For example, the PRAISE-HK app offers real-time and forecasted high-resolution (hourly) health risk information that is related to the air pollution at a street-by-street level [50]. However, our recent study demonstrated that the long-term trend in AR for a mixture of outdoor PM10, NO2, O3, and SO2 concentrations from 2000 to 2018 has decreased over Hong Kong because of the various emission control measures implemented by the Hong Kong government [33].
The longitudinal study design of the study provided an opportunity to quantify the inter- and intra-individual variability and the contributors of variability in terms of daily health risk. The results demonstrated that inter- and intra- individual variability in TIARcombine is almost equally important. Among the identified key contributors for intra-individual variability, PM2.5, NO2 and O3 concentration in ‘home indoor’, O3 in ‘office indoor’ and ambient PM2.5 concentrations were significantly correlated with TIARcombine by a correlation coefficient, r > 0.50. Thus, by reducing indoor sources and infiltrated ambient concentrations of PM2.5, NO2 and O3 in the home, O3 concentration at the office, and exposure to ambient PM2.5 concentrations, people can reduce health risk in their daily life, such as hospital admissions and emergency room visits due to respiratory and cardiovascular diseases. People can reduce the infiltrated ambient concentration at home by changing ventilation operation (i.e., reducing window opening duration, air-condition on) and using an air purifier (i.e., high-efficiency particulate air filter) [56,57,58,59]. Exposure concentration at home can be reduced from indoor sources by reducing cooking duration, not smoking inside the home, using an exhaust fan during and after cooking and using an electric stove [59,60,61,62]. At the office, people can reduce the indoor emission of O3 by not using the photocopier or printer and using an air purifier that produces O3 [63,64,65,66]. Thus, this study argues that current air quality management strategies focusing on single pollution emission sources and ambient air quality are not sufficient for effectively mitigating the public health risk of air pollution. Intra-individual variability in TIAR shows how health risk changes with changes in daily exposure concentrations and an individual’s activities. People can use PRAISE-HK app, that provides personalized information on air pollution exposure and health risk, to check their daily health risk and examine the effects of different interventions by modifying their daily activities and lifestyle to reduce their daily health risk [50]. This study provides an insight into the importance of capturing the day-to-day fluctuation in health risk of a mixture of air pollutants within an individual in future epidemiological studies. This study is new in terms of assessing the inter- and intra-individual variability and the key contributors affecting variability in the daily time-integrated health risk for combined personal exposure to particle and gaseous pollutants.
With the recent technological advancement, we measured high-resolution (1 min) air quality concentrations simultaneously for both particle and gaseous pollutants using an integrated portable sensor across the various microenvironments encountered by the participants. High-resolution personal exposure concentrations and time-location patterns across the various microenvironments provided a better representation of each microenvironment for the health risk of combined personal PM2.5, NO2 and O3 exposure concentrations [20]. Overall, the method based on an epidemiological AR model has been proved to be effective in quantifying the health risk for combined personal PM2.5, NO2 and O3 exposure concentrations across various urban microenvironments. This method provides a valuable reference that can be applied in other cities of the world to estimate personal health risk for a mixture of pollutants across the microenvironments.
The study has some limitations. The study subject sample was small because of: (1) the cost of integrated portable sensors; and (2) participant’s burdens to carry the 15 kg portable sensors all the time with them during the measurement campaign, which prevented the implementation of a large number of samples. Our study subjects were only limited to those who were affiliated to the university (i.e., students, faculty members, and staff). Hence, the results may not be representative of the people who are housewives, unemployed, retired or employed in refinery, chemical plants, and restaurants.
5. Conclusions
The exposure error of gaseous pollutants (i.e., NO2 and O3) based on either a fixed-site monitor or residence location as a surrogate indicates the importance of real world personal exposure concentration measurements with a daily active lifestyle. This study is new in terms of quantifying the health risk for combined personal PM2.5, NO2 and O3 exposure concentrations based on an epidemiological model for respiratory and cardiovascular-related hospitalization across five different microenvironments. Despite a small fraction of time spent, ‘others indoor’, ‘outdoor’ and ‘transit’ microenvironments contribute disproportionately to the daily health risk. Thus, there are potential ways to reduce an individual’s daily health risk related to air pollution by minimizing their exposure time in these microenvironments. The inter- and intra-individual variability in daily time-integrated health risk for PM2.5 was substantially different from the gaseous pollutants. The daily time-integrated health risk for combined PM2.5, NO2, and O3 (TIARcombine) varied by a factor up to 2.5 for a given person across measured days. Several factors were identified to be significantly correlated with daily TIARcombine, with the top five factors including the PM2.5, NO2 and O3 concentrations at ‘home indoor’ microenvironments, O3 concentrations at ‘office indoor’ microenvironments and ambient PM2.5 concentrations. The results on the key contributors of variability in the daily personal health risk for combined PM2.5, NO2, and O3 exposure concentrations can be used to guide developing strategies for reducing an individual’s health effects of air pollution. This study highlights the importance of individual health risk based on real-world exposure to a mixture of air pollutants that policymakers can prioritize in future policy development. This study provides a reference for the method that can be applied in other cities of the world to quantify and evaluate the health risk for combined personal exposure to a mixture of pollutants.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/ijerph19010565/s1, File S1.
Author Contributions
Conceptualization, S.H. and W.C.; methodology, S.H., W.C. and A.K.-H.L.; software, S.H.; validation, S.H.; formal analysis, S.H.; investigation, S.H.; resources, A.K.-H.L.; data curation, W.C. and S.H.; writing—original draft preparation, S.H.; writing—review and editing, W.C.; visualization, S.H.; supervision, W.C. and A.K.-H.L.; project administration, W.C. and A.K.-H.L.; funding acquisition, A.K.-H.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the HSBC 150th Anniversary Charity Programme through the PRAISE-HK project and The APC was funded by the National Natural Science Foundation of China 41703104. The work of the first author was also supported by the Hong Kong PhD Fellowship Scheme.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Human and Artefacts Research Ethics Committee of The Hong Kong University of Science and Technology (protocol code HAREC #595 and approved on 4 February 2021).
Informed Consent Statement
Informed consent was taken from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request to the corresponding author.
Acknowledgments
We would like to thank Henry Christopher Frey at the United States Environmental Protection Agency and North Carolina State University for his helpful comments on this work. We also would like to thank all the participants for participating in this study. We like to thank to aLoggers LLC (aTimeLogger app developer).
Conflicts of Interest
The authors declare no conflict of interest.
References
- WHO. WHO Global Urban Ambient Air Pollution Database (Update 2016), World Health Organization. 2016. Available online: https://www.who.int/airpollution/data/cities-2016/en/ (accessed on 2 April 2021).
- USEPA. Integrated Science Assessment for Particulate Matter; Center for Public Health and Environmental Assessment, Office of Research and Development, United States Environmental Protection Agency: Research Triangle Park, NC, USA, 2019.
- USEPA. Integrated Science Assessment for Oxides of Nitrogen-Health Criteria; National Center for Environmental Assessment-RTP Division, Office of Research and Development, United States Environmental Protection Agency: Research Triangle Park, NC, USA, 2016.
- USEPA. Integrated Science Assessment for Ozone and Related Photochemical Oxidants (External Review Draft); National Center for Environmental Assessment-RTP Division, Office of Research and Development, United States Environmental Protection Agency: Research Triangle, NC, USA, 2019.
- Li, S.; Batterman, S.; Wasilevich, E.; Wahl, R.; Wirth, J.; Su, F.-C.; Mukherjee, B. Association of daily asthma emergency department visits and hospital admissions with ambient air pollutants among the pediatric Medicaid population in Detroit: Time-series and time-stratified case-crossover analyses with threshold effects. Environ. Res. 2011, 111, 1137–1147. [Google Scholar] [CrossRef]
- Dauchet, L.; Hulo, S.; Cherot-Kornobis, N.; Matran, R.; Amouyel, P.; Edmé, J.-L.; Giovannelli, J. Short-term exposure to air pollution: Associations with lung function and inflammatory markers in non-smoking, healthy adults. Environ. Int. 2018, 121, 610–619. [Google Scholar] [CrossRef] [PubMed]
- Myung, W.; Lee, H.; Kim, H. Short-term air pollution exposure and emergency department visits for amyotrophic lateral sclerosis: A time-stratified case-crossover analysis. Environ. Int. 2019, 123, 467–475. [Google Scholar] [CrossRef]
- Tam, W.W.S.; Wong, T.W.; Wong, A.H. Association between air pollution and daily mortality and hospital admission due to ischaemic heart diseases in Hong Kong. Atmos. Environ. 2015, 120, 360–368. [Google Scholar] [CrossRef]
- Tam, W.W.S.; Wong, T.W.; Ng, L.; Wong, S.Y.-S.; Kung, K.K.L.; Wong, A.H.S. Association between Air Pollution and General Outpatient Clinic Consultations for Upper Respiratory Tract Infections in Hong Kong. PLoS ONE 2014, 9, e86913. [Google Scholar] [CrossRef] [Green Version]
- Habre, R.; Coull, B.; Moshier, E.; Godbold, J.; Grunin, A.; Nath, A.; Castro, W.; Schachter, N.; Rohr, A.; Kattan, M.; et al. Sources of indoor air pollution in New York City residences of asthmatic children. J. Expo. Sci. Environ. Epidemiol. 2014, 24, 269–278. [Google Scholar] [CrossRef]
- Che, W.; Frey, H.C.; Li, Z.; Lao, X.; Lau, A.K.H. Indoor Exposure to Ambient Particles and Its Estimation Using Fixed Site Monitors. Environ. Sci. Technol. 2018, 53, 808–819. [Google Scholar] [CrossRef] [PubMed]
- Hoek, G.; Beelen, R.; De Hoogh, K.; Vienneau, D.; Gulliver, J.; Fischer, P.; Briggs, D. A review of land-use regression models to assess spatial variation of outdoor air pollution. Atmos. Environ. 2008, 42, 7561–7578. [Google Scholar] [CrossRef]
- Eeftens, M.; Beelen, R.; de Hoogh, K.; Bellander, T.; Cesaroni, G.; Cirach, M.; Declercq, C.; Dėdelė, A.; Dons, E.; de Nazelle, A.; et al. Development of Land Use Regression Models for PM2.5, PM2.5 Absorbance, PM10 and PM coarse in 20 european study areas; results of the ESCAPE project. Environ. Sci. Technol. 2012, 46, 11195–11205. [Google Scholar] [CrossRef]
- Zhang, J.J.; Sun, L.; Barrett, O.; Bertazzon, S.; Underwood, F.E.; Johnson, M. Development of land-use regression models for metals associated with airborne particulate matter in a North American city. Atmos. Environ. 2015, 106, 165–177. [Google Scholar] [CrossRef]
- Chen, L.; Bai, Z.; Kong, S.; Han, B.; You, Y.; Ding, X.; Du, S.; Liu, A. A land use regression for predicting NO2 and PM10 concentrations in different seasons in Tianjin region, China. J. Environ. Sci. 2010, 22, 1364–1373. [Google Scholar] [CrossRef]
- Mazaheri, M.; Clifford, S.; Yeganeh, B.; Viana, M.; Rizza, V.; Flament, R.; Buonanno, G.; Morawska, L. Investigations into factors affecting personal exposure to particles in urban microenvironments using low-cost sensors. Environ. Int. 2018, 120, 496–504. [Google Scholar] [CrossRef] [PubMed]
- Koehler, K.; Good, N.; Wilson, A.; Mölter, A.; Moore, B.F.; Carpenter, T.; Peel, J.L.; Volckens, J. The Fort Collins commuter study: Variability in personal exposure to air pollutants by microenvironment. Indoor Air 2019, 29, 231–241. [Google Scholar] [CrossRef] [Green Version]
- Ma, J.; Tao, Y.; Kwan, M.-P.; Chai, Y. Assessing Mobility-Based Real-Time Air Pollution Exposure in Space and Time Using Smart Sensors and GPS Trajectories in Beijing. Ann. Am. Assoc. Geogr. 2020, 110, 434–448. [Google Scholar] [CrossRef]
- Watson, A.Y.; Bates, R.R.; Kennedy, D. Assessment of Human Exposure to Air Pollution: Methods, Measurements, and Models. 1988. Available online: https://www.ncbi.nlm.nih.gov/books/NBK218147/ (accessed on 20 June 2021).
- Van Ryswyk, K.; Wheeler, A.J.; Wallace, L.; Kearney, J.; You, H.; Kulka, R.; Xu, X. Impact of microenvironments and personal activities on personal PM2.5 exposures among asthmatic children. J. Expo. Sci. Environ. Epidemiol. 2014, 24, 260–268. [Google Scholar] [CrossRef] [Green Version]
- Kolluru, S.S.R.; Patra, A.K.; Sahu, S.P. A comparison of personal exposure to air pollutants in different travel modes on national highways in India. Sci. Total Environ. 2018, 619–620, 155–164. [Google Scholar] [CrossRef]
- Yang, F.; Lau, C.F.; Tong, V.W.T.; Zhang, K.K.; Westerdahl, D.; Ng, S.; Ning, Z. Assessment of personal integrated exposure to fine particulate matter of urban residents in Hong Kong. J. Air Waste Manag. Assoc. 2018, 69, 47–57. [Google Scholar] [CrossRef]
- Jahn, H.J.; Kraemer, A.; Chen, X.-C.; Chan, C.-Y.; Engling, G.; Ward, T.J. Ambient and personal PM2.5 exposure assessment in the Chinese megacity of Guangzhou. Atmos. Environ. 2013, 74, 402–411. [Google Scholar] [CrossRef]
- Tunno, B.J.; Dalton, R.; Michanowicz, D.R.; Shmool, J.L.C.; Kinnee, E.; Tripathy, S.; Cambal, L.; Clougherty, J.E. Spatial patterning in PM2.5 constituents under an inversion-focused sampling design across an urban area of complex terrain. Expo. Sci. Environ. Epidemiol. 2016, 26, 385–396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, N.; Xu, C.; Liu, Z.; Li, N.; Chartier, R.; Chang, J.; Wang, Q.; Wu, Y.; Li, Y.; Xu, D. Determinants of personal exposure to fine particulate matter in the retired adults—Results of a panel study in two megacities, China. Environ. Pollut. 2020, 265, 114989. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.-C.; Jahn, H.J.; Ward, T.J.; Ho, H.C.; Luo, M.; Engling, G.; Kraemer, A. Characteristics and determinants of personal exposure to PM2.5 mass and components in adult subjects in the megacity of Guangzhou, China. Atmos. Environ. 2020, 224, 117295. [Google Scholar] [CrossRef]
- Chen, X.-C.; Ward, T.J.; Cao, J.-J.; Lee, S.-C.; Chow, J.C.; Lau, G.N.; Yim, S.H.L.; Ho, K.-F. Determinants of personal exposure to fine particulate matter (PM2.5) in adult subjects in Hong Kong. Sci. Total Environ. 2018, 628–629, 1165–1177. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, M.; Milà, C.; Sreekanth, V.; Balakrishnan, K.; Sambandam, S.; Nieuwenhuijsen, M.; Kinra, S.; Marshall, J.D.; Tonne, C. Personal exposure to particulate matter in peri-urban India: Predictors and association with ambient concentration at residence. J. Expo. Sci. Environ. Epidemiol. 2020, 30, 596–605. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.; Bartell, S.M.; Paek, M. Interpersonal and daily variability of personal exposures to nitrogen dioxide and sulfur dioxide. J. Expo. Sci. Environ. Epidemiol. 2004, 14, 137–143. [Google Scholar] [CrossRef] [Green Version]
- Grivas, G.; Dimakopoulou, K.; Samoli, E.; Papakosta, D.; Karakatsani, A.; Katsouyanni, K.; Chaloulakou, A. Ozone exposure assessment for children in Greece-Results from the RESPOZE study. Sci. Total Environ. 2017, 581–582, 518–529. [Google Scholar] [CrossRef]
- Wong, T.W.; Tam, W.; Yu, I.T.S.; Lau, A.; Pang, S.W.; Wong, A.H. Developing a risk-based air quality health index. Atmos. Environ. 2013, 76, 52–58. [Google Scholar] [CrossRef]
- HKEPD. Air Quality Health Index-Frequently Asked Questions. Environmental Protection Department, Hong Kong, 2019. Available online: http://www.aqhi.gov.hk/en/what-is-aqhi/faqs.html#e_05 (accessed on 14 October 2019).
- Hossain, S.; Frey, H.C.; Louie, P.K.; Lau, A.K. Combined effects of increased O3 and reduced NO2 concentrations on short-term air pollution health risks in Hong Kong. Environ. Pollut. 2021, 270, 116280. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.C.; Cheng, Y.; Ho, K.F.; Cao, J.J.; Louie, P.K.-K.; Chow, J.C.; Watson, J. PM1.0 and PM2.5 characteristics in the roadside environment of Hong Kong. Aerosol Sci. Technol. 2006, 40, 157–165. [Google Scholar] [CrossRef] [Green Version]
- Che, W.; Tso, C.Y.; Sun, L.; Ip, D.Y.; Lee, H.; Chao, Y.H.C.; Lau, A.K. Energy consumption, indoor thermal comfort and air quality in a commercial office with retrofitted heat, ventilation and air conditioning (HVAC) system. Energy Build. 2019, 201, 202–215. [Google Scholar] [CrossRef]
- Sun, L.; Wong, K.C.; Wei, P.; Ye, S.; Huang, H.; Yang, F.; Westerdahl, D.; Louie, P.K.; Luk, C.W.; Ning, Z. Development and application of a next generation air sensor network for the Hong Kong marathon 2015 air quality monitoring. Sensors 2016, 16, 211. [Google Scholar] [CrossRef]
- Sun, L.; Westerdahl, D.; Ning, Z. Development and evaluation of a novel and cost-effective approach for low-cost NO2 sensor drift correction. Sensors 2017, 17, 1916. [Google Scholar] [CrossRef] [PubMed]
- Che, W.; Li, A.T.Y.; Frey, H.C.; Tang, K.T.J.; Sun, L.; Wei, P.; Hossain, S.; Hohenberger, T.L.; Leung, K.W.; Lau, A.K.H. Factors affecting variability in gaseous and particle microenvironmental air pollutant concentrations in Hong Kong primary and secondary schools. Indoor Air 2020, 31, 170–187. [Google Scholar] [CrossRef]
- Hossain, S.; Che, W.; Frey, H.C.; Lau, A.K. Factors affecting variability in infiltration of ambient particle and gaseous pollutants into home at urban environment. Build. Environ. 2021, 206, 108351. [Google Scholar] [CrossRef]
- Persily, A.K. Evaluating building IAQ and ventilation with indoor carbon dioxide. ASHRAE Trans. 1997, 103, 193–204. [Google Scholar]
- Satish, U.; Mendell, M.J.; Shekhar, K.; Hotchi, T.; Sullivan, D.; Streufert, S.; Fisk, W.J. Is CO2 an Indoor Pollutant? Direct Effects of Low-to-Moderate CO2 Concentrations on Human Decision-Making Performance. Environ. Health Perspect. 2012, 120, 1671–1677. [Google Scholar] [CrossRef] [Green Version]
- Klepeis, N.E. An introduction to the indirect exposure assessment approach: Modeling human exposure using microenvironmental measurements and the recent National Human Activity Pattern Survey. Environ. Health Perspect. 1999, 107, 365–374. [Google Scholar] [CrossRef] [PubMed]
- Mazaheri, M.; Clifford, S.; Jayaratne, R.; Mokhtar, M.A.M.; Fuoco, F.; Buonanno, G.; Morawska, L. School children’s personal exposure to ultrafine particles in the urban environment. Environ. Sci. Technol. 2013, 48, 113–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, R. Measuring explained variation in linear mixed effects models. Stat. Med. 2003, 22, 3527–3541. [Google Scholar] [CrossRef]
- Sahai, H.; Ageel, M.I. The Analysis of Variance: Fixed, Random, and Mixed Models; Birkhäuser: Boston, MA, USA, 2000. [Google Scholar]
- Xu, M.; Sbihi, H.; Pan, X.; Brauer, M. Local variation of PM2.5 and NO2 concentrations within metropolitan Beijing. Atmos. Environ. 2019, 200, 254–263. [Google Scholar] [CrossRef]
- Squizzato, S.; Masiol, M.; Rich, D.Q.; Hopke, P.K. PM2.5 and gaseous pollutants in New York State during 2005–2016: Spatial variability, temporal trends, and economic influences. Atmos. Environ. 2018, 183, 209–224. [Google Scholar] [CrossRef]
- Baxter, L.K.; Clougherty, J.E.; Laden, F.; Levy, J.I. Predictors of concentrations of nitrogen dioxide, fine particulate matter, and particle constituents inside of lower socioeconomic status urban homes. J. Expo. Sci. Environ. Epidemiol. 2007, 17, 433–444. [Google Scholar] [CrossRef] [Green Version]
- Schober, P.; Boer, C.; Schwarte, L.A. Correlation coefficients: Appropriate use and interpretation. Anesth. Analg. 2018, 126, 1763–1768. [Google Scholar] [CrossRef]
- Che, W.; Frey, H.C.; Fung, J.C.; Ning, Z.; Qu, H.; Lo, H.K.; Chen, L.; Wong, T.-W.; Wong, M.K.; Lee, O.C.; et al. PRAISE-HK: A personalized real-time air quality informatics system for citizen participation in exposure and health risk management. Sustain. Cities Soc. 2020, 54, 101986. [Google Scholar] [CrossRef]
- IQAir. IQAir | The World’s Leading Air Quality App. 2021. Available online: https://www.iqair.com/air-quality-app (accessed on 4 June 2021).
- BreezoMeter. Accurate Air Quality, Pollen & Active Fires Information|BreezoMeter. 2021. Available online: https://www.breezometer.com/ (accessed on 4 June 2021).
- AirMatters. Air Matters—A Global Air Quality Service Provider. 2021. Available online: https://air-matters.com/index.html (accessed on 4 June 2021).
- USDOS. ZephAir App Available Now—United States Department of State. 2021. Available online: https://www.state.gov/zephair-app-available-now/ (accessed on 4 June 2021).
- PlumeLabs. Plume Labs App: Live and Forecast air Quality Data. 2021. Available online: https://plumelabs.com/en/air/ (accessed on 4 June 2021).
- Allen, R.W.; Adar, S.D.; Avol, E.; Cohen, M.; Curl, C.L.; Larson, T.; Liu, L.-J.S.; Sheppard, L.; Kaufman, J. Modeling the Residential Infiltration of Outdoor PM 2.5 in the Multi-Ethnic Study of Atherosclerosis and Air Pollution (MESA Air). Environ. Health Perspect. 2012, 120, 824–830. [Google Scholar] [CrossRef] [Green Version]
- Zhou, X.; Cai, J.; Zhao, Y.; Chen, R.; Wang, C.; Zhao, A.; Yang, C.; Li, H.; Liu, S.; Cao, J.; et al. Estimation of residential fine particulate matter infiltration in Shanghai, China. Environ. Pollut. 2016, 233, 494–500. [Google Scholar] [CrossRef]
- Xu, C.; Li, N.; Yang, Y.; Li, Y.; Liu, Z.; Wang, Q.; Zheng, T.; Civitarese, A.; Xu, D. Investigation and modeling of the residential infiltration of fine particulate matter in Beijing, China. J. Air Waste Manag. Assoc. 2017, 67, 694–701. [Google Scholar] [CrossRef] [PubMed]
- MacNeill, M.; Wallace, L.; Kearney, J.; Allen, R.; Van Ryswyk, K.; Judek, S.; Xu, X.; Wheeler, A. Factors influencing variability in the infiltration of PM 2.5 mass and its components. Atmos. Environ. 2012, 61, 518–532. [Google Scholar] [CrossRef]
- Dėdelė, A.; Miškinytė, A. Seasonal variation of indoor and outdoor air quality of nitrogen dioxide in homes with gas and electric stoves. Environ. Sci. Pollut. Res. 2016, 23, 17784–17792. [Google Scholar] [CrossRef] [PubMed]
- Dobbin, N.A.; Sun, L.; Wallace, L.; Kulka, R.; You, H.; Shin, T.; Aubin, D.; St-Jean, M.; Singer, B.C. The benefit of kitchen exhaust fan use after cooking—An experimental assessment. Build. Environ. 2018, 135, 286–296. [Google Scholar] [CrossRef]
- Hu, Y.; Zhao, B. Relationship between indoor and outdoor NO2: A review. Build. Environ. 2020, 180, 106909. [Google Scholar] [CrossRef]
- Huang, Y.; Yang, Z.; Gao, Z. Contributions of indoor and outdoor sources to ozone in residential buildings in Nanjing. Int. J. Environ. Res. Public Health 2019, 16, 2587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.-C.; Lam, S.; Fai, H.K. Characterization of VOCs, ozone, and PM10 emissions from office equipment in an environmental chamber. Build. Environ. 2001, 36, 837–842. [Google Scholar] [CrossRef]
- Britigan, N.; Alshawa, A.; Nizkorodov, S.A. Quantification of ozone levels in indoor environments generated by ionization and ozonolysis air purifiers. J. Air Waste Manag. Assoc. 2006, 56, 601–610. [Google Scholar] [CrossRef] [Green Version]
- Guo, C.; Gao, Z.; Shen, J. Emission rates of indoor ozone emission devices: A literature review. Build. Environ. 2019, 158, 302–318. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).